- 30 May, 2026
- Dr. Arun Rajeswaran
- No comment
Spinal Stenosis Explained: Why the Spinal Canal Narrows and What Can Be Done About It
Spinal stenosis is one of the most common spinal conditions in adults over 50, and one of the most commonly missed.
Patients often live with the symptoms for years, gradually adjusting their lives around them. Walking distances shorten. Standing for any length of time becomes uncomfortable. Leaning over a shopping trolley helps, without knowing why.
These adaptations are clues. And recognising them leads to a diagnosis that, in many patients, is very treatable.
What Spinal Stenosis Is
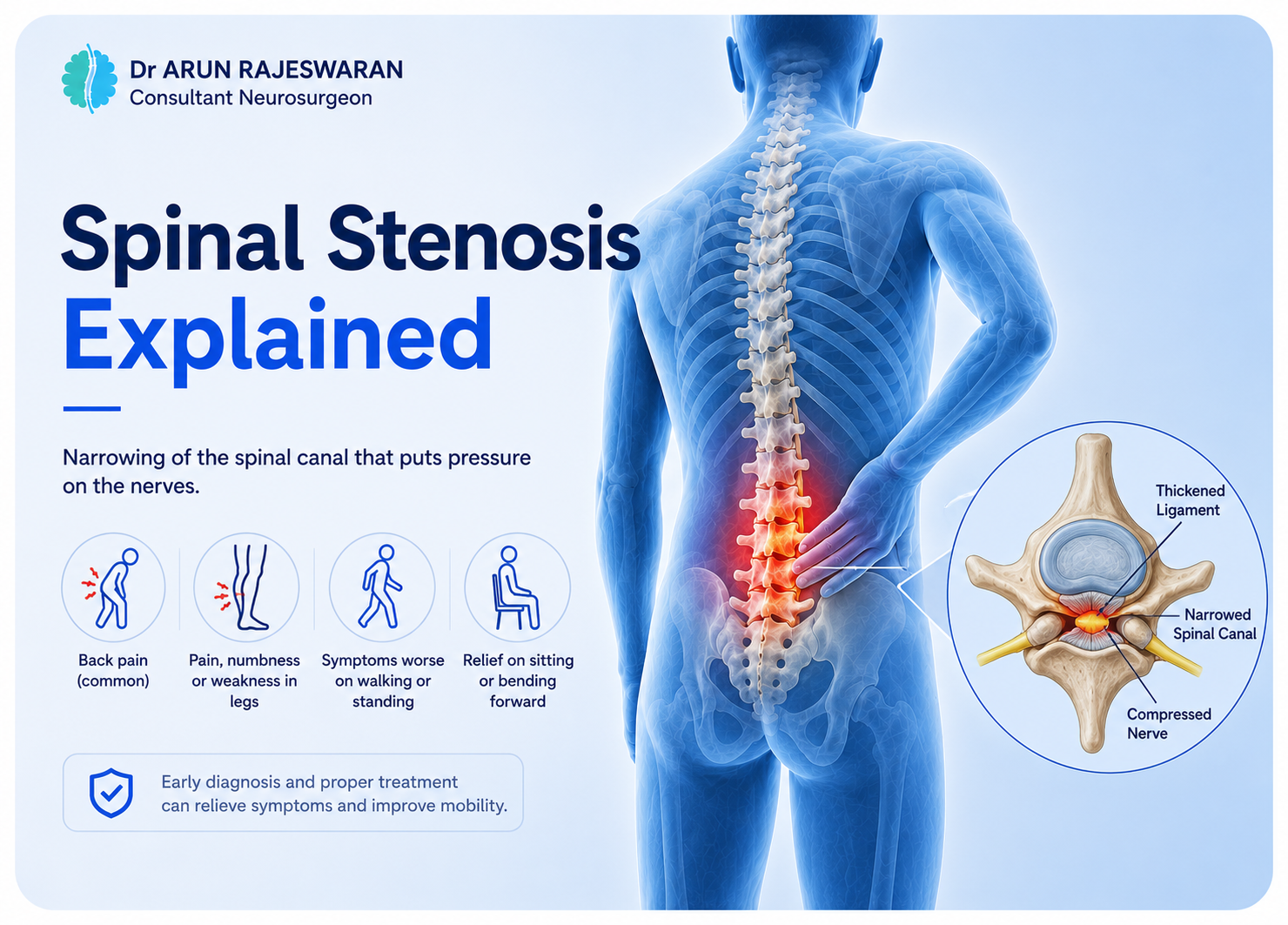
The spinal canal is the tunnel running through the centre of the spine, housing the spinal cord and nerve roots. In a healthy spine, this canal provides comfortable space for the neural structures inside it.
Spinal stenosis is a narrowing of that canal. As the available space shrinks, the neural structures inside become compressed. When they are compressed, they produce symptoms.
Stenosis can occur in the lumbar spine, the cervical spine, or both. Lumbar stenosis is by far the more common presentation, particularly in older adults. Cervical stenosis is less common but more serious when it develops, because cord compression in the neck can cause widespread neurological problems.
What Causes the Narrowing
In the vast majority of adults, spinal stenosis develops as a result of ageing-related degenerative changes.
Discs degenerate and lose height over time. As they collapse, the space at the disc level narrows. The facet joints, the small articulations at the back of each vertebral level, develop arthritis and enlarge. The ligamentum flavum, a ligament running along the back of the spinal canal, thickens and buckles inward as it loses elasticity.
Each of these changes takes up space inside the canal. In combination, they can reduce a canal that was once spacious to one that is critically narrow.
Bone spurs from the degenerating discs and facet joints can grow into the canal and the exit points for individual nerve roots, called the foramina. This is called foraminal stenosis, and it compresses specific nerve roots in addition to the canal narrowing overall.
Less commonly, stenosis can be present from birth if the canal was naturally narrow to begin with. This congenital narrowing means that smaller degenerative changes trigger symptoms earlier than they would in someone with a wider native canal.
What Lumbar Spinal Stenosis Feels Like
The clinical presentation of lumbar stenosis has a characteristic pattern that is quite different from disc herniation or simple back pain.
The defining feature is neurogenic claudication. Back pain and leg symptoms heaviness, aching, cramping, or numbness come on with walking or standing and are relieved by sitting or leaning forward. The distance a patient can walk before symptoms force them to stop is called the claudicant distance. In moderate stenosis, this might be a few hundred metres. In severe cases, it can be much shorter.
Leaning forward or sitting flexes the lumbar spine, which opens the spinal canal and reduces pressure on the nerves. This is why patients unconsciously adopt a forward-flexed posture when standing. Walking uphill, which naturally flexes the spine, is often easier than walking on a flat surface.
Back pain is usually present but is often not the dominant complaint. The leg symptoms bilateral or alternating are what limit patients most. Some describe the legs as feeling heavy or wooden after walking. Some experience burning or tingling. Some say the legs simply stop working properly.
It is important to distinguish neurogenic claudication from vascular claudication, which is calf pain from arterial insufficiency. Both cause pain with walking that is relieved by rest. Vascular claudication is relieved by standing still. Neurogenic claudication requires sitting or bending forward to ease. The distinction matters because the treatment is completely different.
Cervical Stenosis: A More Serious Situation
When narrowing occurs in the cervical spine and compresses the spinal cord, the consequences are more far-reaching.
Cervical stenosis can cause myelopathy, the syndrome of spinal cord dysfunction described in the cervical disc article. Clumsiness of the hands, difficulty with fine movements, heavy or stiff legs, balance problems, and bladder changes can all result.
Unlike lumbar stenosis, where the symptoms mainly affect walking and comfort, cervical myelopathy from cord compression can affect the entire body below the level of the compression. And unlike lumbar stenosis, where a conservative approach is often reasonable first, significant cervical cord compression with neurological signs usually warrants surgical decompression to prevent deterioration.
Diagnosing Spinal Stenosis
The clinical history and examination give strong diagnostic clues before imaging is done. The pattern of symptoms with walking and their relief with flexion is fairly specific.
MRI of the lumbar or cervical spine confirms the diagnosis, shows the degree of canal narrowing, identifies which levels are affected, and demonstrates any cord signal change in cervical cases, which indicates cord damage.
Standing or dynamic X-rays can assess spinal alignment and any instability, which is relevant for surgical planning.
Conservative Treatment
Mild to moderate stenosis with manageable symptoms can often be treated non-surgically for a significant period.
Physiotherapy focuses on flexion-based exercises that strengthen the core, reduce lumbar lordosis during activity, and teach posture strategies that reduce symptoms. Extension-based exercises tend to worsen lumbar stenosis symptoms and should be avoided.
Activity modification helps. Swimming and cycling are generally well-tolerated because both involve a flexed spinal position. Walking with a shopping trolley, a walking frame, or trekking poles, all of which allow a slightly forward-leaning posture, can extend walking distance significantly.
Epidural steroid injections can reduce inflammation and provide meaningful relief for weeks to months. They do not change the structural stenosis, but they can significantly improve quality of life during the period of conservative management.
Pain management with anti-inflammatories, nerve agents, and muscle relaxants follows the same principles as other spinal conditions.
Surgery for Spinal Stenosis
When conservative treatment is no longer managing symptoms adequately, when walking distance has become severely limited, or when neurological signs are developing, surgery offers reliable improvement.
The standard operation for lumbar stenosis is a laminectomy or laminotomy. This involves removing the thickened bone and ligament compressing the nerves, creating more space within the canal. It is done through the back, usually under general anaesthesia.
Minimally invasive variants of this procedure, including tubular or endoscopic approaches, reduce tissue disruption and can offer faster recovery in appropriate patients.
If spinal instability or deformity is present alongside the stenosis, instrumented fusion adding pedicle screws and rods to stabilize the spine is performed at the same time.
Results from surgery for lumbar stenosis are generally good. Most patients experience significant improvement in leg symptoms and walking tolerance. Back pain response is more variable.
For cervical stenosis causing myelopathy, an anterior or posterior decompression is performed, with or without fusion, depending on the extent and location of the narrowing.
Frequently Asked Question
Lumbar stenosis typically produces back pain and leg symptoms of heaviness, aching, tingling, or numbness that come on after walking or standing for a period and ease when sitting or bending forward. The legs may feel heavy or unreliable. Symptoms are often bilateral. The distance a patient can walk before needing to stop gradually shortens as stenosis progresses. Cervical stenosis from cord compression feels different: hand clumsiness, leg stiffness, balance changes, and sometimes bladder symptoms, reflecting widespread cord dysfunction rather than localised nerve root irritation.
Yes, in most cases. The degenerative changes that cause stenosis are progressive. Canal narrowing tends to increase gradually over years. Symptoms may remain stable for long periods and then worsen, or they may progress more steadily. Some patients note a slow but consistent reduction in how far they can walk or how long they can stand. Cervical stenosis causing myelopathy tends to be more consistently progressive. This is why monitoring and timely treatment planning matter, particularly when neurological signs develop.
It is the defining symptom for most patients with lumbar stenosis. Walking a limited distance before leg symptoms force a rest is characteristic, and this claudicant distance tends to shorten as the condition progresses. Many patients find strategies that help, such as using a trolley, leaning slightly forward, or adopting a walking frame. These work by flexing the spine and opening the canal slightly. Cycling and swimming are often tolerated better than walking because both involve a flexed spinal posture.
Surgery is appropriate when conservative treatment is no longer managing symptoms adequately, when walking tolerance has become severely limited, or when neurological signs such as leg weakness are developing. For cervical stenosis causing myelopathy, early surgical decompression is usually recommended because waiting for significant neurological deterioration makes recovery less complete. For lumbar stenosis, there is more flexibility in timing, but prolonged conservative management in a patient whose quality of life is significantly affected is not always in their best interest.
Many patients with lumbar stenosis manage well with conservative treatment for years. Physiotherapy, activity modification, epidural injections, and appropriate pain management can provide meaningful quality of life without surgery. The key is that conservative treatment manages symptoms and does not reverse the stenosis. When symptoms are becoming unmanageable or neurological deterioration appears, surgery becomes the more appropriate choice. Cervical stenosis with cord compression is less suited to long-term conservative management because of the progressive risk to the spinal cord.